



Contents
Scroll to:
https://doi.org/10.47183/mes.2025-375
Scroll to:
Introduction. Recent observations indicate that craniofacial injuries can present as isolated, multiple, or combined trauma. Currently, there is a lack of objective criteria for determining impairments of vital functions that necessitate specialized, multidisciplinary medical care at Level I trauma centers, including multistage surgical treatment (MST) as a criterion for comprehensive management. Furthermore, criteria and indications for the comprehensive treatment of combined injuries, which account for up to 80% of cases, have not been developed in sufficient detail.
Objective. Development of a rational MST protocol for combined trauma that takes into account injury severity and impaired body functions in patients with midface injuries.
Materials and methods. A total of 132 patients were examined, with males comprising 84.8% (n = 112) and females comprising 15.2% (n = 20). The age distribution of the patients was as follows: males aged 20–39 years — 44.7% (n = 59), males aged 40–59 years — 40.1% (n = 53); females aged 20–39 years — 1.5% (n = 2), females aged 40–59 years — 13.6% (n = 18). All patients were divided into three groups: Group 1 — 40 patients (30 males; 10 females) with a compensated course (trauma disease (TD) Type I); Group 2 — 44 patients (38 males; 6 females) with a subcompensated course (TD Type II); Group 3 — 48 patients (44 males; 4 females) with a decompensated course (TD Type III). The study outcomes were assessed based on injury severity and impaired body functions. Injury severity was evaluated using the Trauma Shock Potential Scale (Tsibin), the Military Field Surgery — Injury Scale (MFS-I), and the Abbreviated Injury Scale (AIS). Impaired body functions were evaluated using MFS-SE (State Upon Entry), MFS-SA (State After Admission), and MFS-SS (Specialized State) scales. Statistical data processing was performed using the Statistica 10 software package. Standard descriptive statistics were calculated (mean [M], standard deviation [SD], median [Me], lower [Q1] and upper [Q3] quartiles). Hypothesis testing for the equality of means was assessed using Student’s t-test.
Results. The conducted analysis of statistical data on the nature of injuries and impaired vital body functions allowed an MST methodology to be developed. Its application enabled adequate administration of specialized resuscitative care in 90% of cases, as well as multidisciplinary surgical care. For Group 1 patients, MST was primarily provided on an abbreviated basis, without performing a tracheostomy or gastrostomy, followed by a full-scale surgical intervention during the first period of TD. Treatment for patients in Groups 2 and 3 was initiated in a shock room or an intensive care unit (ICU).
Conclusions. In cases of TD Type I, i.e., isolated maxillofacial injury with a compensated course, the principles and algorithms of the general therapeutic and tactical approach to TD management are not applicable, and the full scope of surgical interventions can be performed during the first period of TD. In cases of TD Types II and III, the full scope of MST should be implemented.
Shcherbuk Yu.A., Madai O.D., Madai D.Yu., Shcherbuk A.Yu. Multistage surgical management of patients with combined craniofacial injuries. Extreme Medicine. 2026;28(1):123-133. https://doi.org/10.47183/mes.2025-375
Multistage surgical treatment (MST) is the cornerstone of management for patients with midface injuries. This approach is based on assessing the severity of the patient’s general condition and evaluating the level of compensation for impaired body functions. The MST includes the following three stages: primary emergency surgery on a limited basis (abbreviated); intensive therapy until stabilization of vital body functions; and repeated surgical intervention to correct the remaining injuries. Currently, adequate standardized algorithms for MST are lacking [1–3].
The refinement of MST for patients with combined craniofacial trauma remains a critical challenge in trauma surgery. The relevance of this issue is underscored by the high mortality rate observed in these patients. In the late 20th century, the Early Total Care (ETC) system was proposed, which advocated for the treatment of all injuries within the first 24 h. However, the ETC system cannot be considered versatile; moreover, its use does not lead to a reduction in mortality [4–7].
Recently, new approaches for the treatment of severe mechanical trauma based on the damage control strategy have been developed [7][8]. Three types of this strategy can be distinguished:
According to V.A. Sokolov, immunological studies have confirmed that trauma induces a local inflammatory response (LIR) with increased concentrations of pro-inflammatory cytokines. This cascade of changes leads to the development of a condition referred to as the Multiple Organ Dysfunction Syndrome (MODS) in the Western scientific literature. In Russian publications, it is called the Disseminated Intravascular Coagulation (DIC) syndrome.2
MST is applied when it is possible to assess the severity of trauma, the general condition of the organism, the number of surgical interventions required, and their potential outcome [1][7–10]. Such a multistage approach is a treatment strategy of choice for critical conditions, involving only those methods which do not worsen the status of patients with varying degrees of general condition severity, as assessed based on objective indicators.
The foundation of specialized, multidisciplinary medical care for severe combined craniofacial trauma consists in resuscitative measures and multistage surgical assistance. This integrated approach enables the creation of a therapeutic and tactical scheme for comprehensive treatment, spanning from the moment of admission to a shock room through to the rehabilitation period. The advantage of this approach, in contrast to the “damage control” strategy, lies in the fact that MST is based both on damage control during the execution of Stages 1 and 2, as well as on performing restorative surgical interventions during the rehabilitation period.
At the beginning of the 21st century, the Russian healthcare system face two major challenges. These were the implementation of a new national healthcare system and the integration of a system for emergency specialized multidisciplinary medical care into regional healthcare. This new system integrates prehospital specialized care with Level I and Level II regional trauma centers to provide emergency specialized multidisciplinary medical assistance. This framework allows for the execution of specific elements of MST at Level II trauma centers (e.g., temporary control of ongoing external hemorrhage, management of asphyxia by cricothyrotomy and tracheostomy).
Severe combined trauma requires emergency specialized multidisciplinary medical care, including specialized resuscitative care in intensive care units (ICUs) and emergency multidisciplinary specialized surgical care (MSSC) in operating rooms. Specialized resuscitative care involves addressing several objectives: (1) restoration of circulating blood volume, (2) maintenance of adequate circulation, and (3) respiratory therapy. Emergency MSSC is provided in full in shock rooms. One-third of all surgeries are performed under delayed emergency indications, while one-fifth are urgent surgeries [1]. A crucial aspect in the management of severe combined trauma is the provision of the full scope of emergency multidisciplinary specialized surgical care in the form of MSSC.
In the ICU, the Military Field Surgery — State After Admission (MFS-SA) scale is used for the dynamic assessment of the severity of physiological function impairments (i.e., the severity of the patient’s condition). Subsequently, the Military Field Surgery — Specialized State (MFS-SS) scale is applied. This scale enables the diagnosis of endotoxicosis, multiple organ failure, acute lung injury syndrome, and systemic inflammatory response syndrome.
In this study, we aim to develop a methodology of MST for combined midface injuries, taking into account the trauma severity and impaired body functions.
A total of 132 patients were examined, with 84.8% (n = 112) of males and 15.2% (n = 20) of females. The age distribution was as follows: males aged 20–39 years — 44.7% (n = 59), males aged 40–59 years — 40.1% (n = 53); females aged 20–39 years — 1.5% (n = 2), females aged 40–59 years — 13.6% (n = 18). The patients were admitted from the combined trauma departments of Level I trauma centers: the Dzhanelidze Research Institute for Emergency Medicine, the Alexandrovskaya Hospital, and the Military Field Surgery Department of the Kirov Military Medical Academy.
Injury severity criteria were assessed using the following scales:
The following scales were used to assess functional impairments: Military Field Surgery — State Upon Entry (MFS-SE); Military Field Surgery — State After Admission (MFS-SA); Military Field Surgery — Specialized State (MFS-SS) [1][7].
All patients were divided into three groups:
The patients were comparable in terms of sex, age, nature of traumatic injury, structure of combined injuries, and severity of blood loss.
The study outcomes were assessed using the following parameters: injury severity (using the Trauma Shock Potential Scale (Tsibin scale), MFS-I scale, and AIS) and impaired body functions (MFS-SE, MFS-SA, and MFS-SS).
Statistical data processing was performed using the Statistica 10 software. Standard descriptive statistics were calculated (mean [M], standard error of the mean [SEM], median [Me], lower [Q1] and upper [Q3] quartiles). The significance of differences in quantitative variables between independent groups was determined using Student’s t-test (for normally distributed variables).
During the study, in 40 patients with TD Type I (Group 1), the severity of injuries was assessed upon admission using the MFS-I scale at 1.0–2.0 points, and the degree of impaired functions was assessed at 18.8 ± 0.9 points on the MFS-SE scale. Following the performance of emergency and urgent surgical interventions, a rapid decrease in the condition severity index, calculated according to the MFS-SS methodology, was observed.
Simultaneously, in 44 patients (Group 2) with TD Type II, the second period of trauma became distinctly manifest on Day 2 after the injury. This was accompanied by the minimum value of the condition severity index over a 10-day period (MFS-SS — 47.5 ± 0.3 points).
In 48 patients with TD Type III, the trauma disease had the most severe manifestation (complex trauma with impairment of vital functions — polytrauma). The injury severity in this subgroup ranged 19.0–45.5 points on the MFS-I scale (averaging 26.2 ± 0.8 points). The minimum severity of the condition upon admission was 32.0 points on the MFS-SE scale, and the maximum was 75.0 points (Fig. 1).
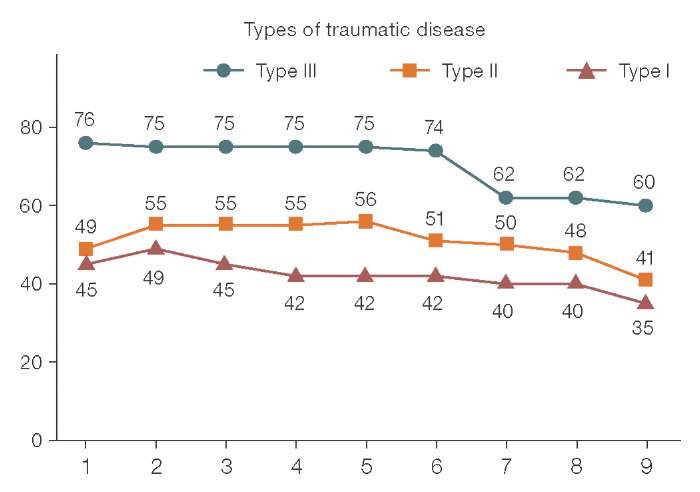
Figure prepared by the authors based on original data
Fig. 1. Daily score dynamics of the general condition of patients in the study groups according to the MFS-SS Scale (Military Field Surgery — Specialized State): X-axis — observation day; Y-axis — condition severity score (MFS-SS scale)
The algorithm for diagnosing and treating combined craniofacial injuries was implemented based on a standard fixed parameter (injury severity) and a variable parameter (severity of impaired body functions). Clinical criteria for patient distribution are presented in Tables 1 and 2.
Table 1 presents the criteria for patient hospitalization based on the assessment of the general condition severity using the MFS-SE and MFS-SA scales.
Table 2 presents the injury severity scores for the patients.
Table 1. Qualitative and quantitative parameters of trauma
|
Conventional classification of impaired functions severity |
Scales |
Scoring characterization of impaired functions severity |
Lethality (%) |
Complication rate (%) |
|
Mild |
MFS-SE MFS-SA MFS-SS |
12 16–22 27–32 |
0 0 0 |
0 0 0 |
|
Moderate |
MFS-SE MFS-SA MFS-SS |
13–20 23–32 33–49 |
<3.5 <3.5 <7.5 |
34.0 <34.0 <27.5 |
|
Severe |
MFS-SE MFS-SA MFS-SS |
21–31 33–40 50–69 |
<38.0 <38.0 <32.0 |
<66.0 <66.0 <62.7 |
|
Extremely Severe |
MFS-SE MFS-SA MFS-SS |
32–45 41–50 70–98 |
<84.0 <84.0 <75.0 |
<90.0 <90.0 <86.3 |
|
Critical |
MFS-SE MFS-SA MFS-SS |
>45 >50 >99 |
100 100 100 |
– – – |
Table compiled by the authors based on original data
Note: MFS-SE — Military Field Surgery — State Upon Entry; MFS-SA — Military Field Surgery — State After Admission; MFS-SS — Military Field Surgery — Specialized State.
Table 2. Injury severity scores in patients
|
Injury type |
Scales |
||
|
AIS |
Tsibin scale |
MFS-I |
|
|
Soft tissue wounds of the head |
1 |
- |
0.05 |
|
Closed nasal bone fracture |
1 |
1.5 |
0.2 |
|
Brain concussion |
1 |
0.1 |
0.2 |
|
Jaw fractures |
2 |
1.5 |
0.3 |
|
Mild cerebral contusion |
2 |
0.1 |
0.3 |
|
Moderate brain contusion with calvarial fractures |
2 |
0.5 |
0.5 |
|
Moderate brain contusion with closed fractures of the calvaria and skull base |
3 |
6 |
0.6 |
|
Fractures of the calvaria and skull base (open type), traumatic brain injury (TBI), brain contusion |
4 |
6 |
2 |
|
Brain compression associated with non-severe contusions |
5 |
1 |
7 |
|
Severe brain contusion with injury to the upper brainstem |
5 |
4 |
12 |
|
Brain compression on a background of severe contusions |
5 |
- |
18 |
|
Severe brain contusion with injury to the lower brainstem |
5 |
2 |
19 |
Table complied by the authors based on original data
Note: AIS — Abbreviated Injury Scale; MFS-I — Military Field Surgery — Injury.
In accordance with the requirements of MST, we performed the following measures in the treatment of patients [8][9]:

Images prepared by the authors based on original data
Fig. 2. Anatomy of midface injuries requiring multistage surgical treatment in the rehabilitation period
The photographs (Fig. 2) show defects in the orbital, nasal, and maxillofacial regions that require the full scope of plastic and reconstructive surgical interventions to correct the sequelae of trauma during the rehabilitation period.
Comprehensive surgical treatment for combined craniofacial trauma was performed using a methodology based on the clinical and pathogenetic manifestations of TD and its stages of progression [8][9]. When implementing the developed MST approach according to the compensation level for impaired body functions, we used the MFS-SS scale and the protocol of Military Field Surgery Department of the Kirov Military Medical Academy. According to this framework, the entire MST algorithm was to be carried out.3
Table 3. Compensation variants for impaired functions according to the Military Field Surgery Scale
|
Petameter |
Compensated course of TD Type I |
Subcompensated course of TD Type II |
Decompensated course of TD Type III |
|
Inotropic support |
not administered |
not administered |
administered |
|
Systolic BP (mm Hg) |
100 |
81–100 |
≤ 80 |
|
HR (beats/min) |
60–90 |
91–140 |
< 60 or > 140 |
|
Hematocrit (%) |
31 |
26–31 |
20–25 |
|
Hemoglobin (g/L) |
99 |
85–99 |
60–84 |
|
Erythrocytes (×10¹²/L) |
2.9 |
2.6–2.9 |
2.5 |
|
MFS-SS, points |
50 |
50–69 |
70–98 |
Table complied by the authors based on original data
Note: TD — traumatic disease; BP — blood pressure; MFS-SS — Military Field Surgery — Specialized State.
At the initial stage of managing patients with combined midface injuries, the compensation level for impaired functions was assessed. Upon identifying signs of subcompensation or decompensation, MST was performed under an emergency protocol. This protocol involved providing emergency care in a shock room, followed by transfer to a specialized department for continued treatment after stabilization of the general condition. Upon admission, it is crucial to assess the nature of impaired functions [13–15]. In a decompensated course of the disease, the full scope of Stage 1 MST must be performed. In a subcompensated course of TD, the full scope of Stage 2 MST measures is required. In a compensated course of TD, surgical interventions according to Stage 3 MST can be performed immediately upon admission. Table 4 presents the variants of TD course.
Table 4. Clinical variants of trauma disease course in patients
|
Parameters |
TD Type I (Compensated) |
TD Type II (Subcompensated) |
TD Type III (Decompensated) |
|
Absolute number of patients |
40 (30.3%) |
44 (33.3%) |
48 (36.4%) |
|
Injury Severity by MFS-I Scale, points |
2.8 ± 0.4 |
11.2 ± 1.0* |
17.9 ± 1.3* |
|
State Severity Upon Admission by MFS-SE Scale, points |
18.8 ± 0.9 |
26.2 ± 0.8* |
42.2 ± 3.3* |
|
Incidence of sepsis, abs. number (%) |
– |
8 (18.2%) |
10 (20.8%) |
|
Incidence of septic shock, abs. number (%) |
– |
1 (2.5%) |
5 (10.4%) |
|
Incidence of acute lung injury syndrome, abs. number (%) |
4 (10%) |
5 (10.4%) |
10 (20.8%) |
|
Incidence of acute respiratory distress syndrome, abs. number (%) |
– |
4 (9.09%) |
10 (20.8%) |
|
Incidence of other life-threatening complications (pulmonary embolism, fat embolism syndrome, generalized fibrinolysis), abs. number (%) |
– |
6 (13.6%) |
7 (14.6%) |
|
Lethality, abs. number (%) |
– |
– |
7 (14.6%) |
Table complied by the authors based on original data
Note: MFS-I — Military Field Surgery — Injury; MFS-SE — Military Field Surgery (State Upon Entry); PE — pulmonary embolism; TD — trauma disease; * — differences are statistically significant at p < 0.05.
The analysis of injury severity (MFS-I scale) and general condition (MFS-SE scale) revealed statistically significant differences between TD Types I, II, and III. On this basis, the use of the abbreviated MST protocol was not required, and the full scope of surgical intervention for patients in Group 1 was performed.
In 40 patients from Group 1, following emergency and urgent surgical interventions, a rapid decrease in the condition severity index, calculated using the MFS-SS (Military Field Surgery — Specialized State) methodology, was observed. Within 12 h of hospital admission, its values did not exceed 49 points (moderate severity condition), averaging 45.8 ± 0.3 points. It should be noted that in some patients (19 patients (38.0%)) of this subgroup, the MFS-SS index was already below 49 points within 6 h of hospitalization. Starting from Day 3, the state indicators of the systems indicated persistent subcompensation. In this subgroup of patients, relatively “non-life-threatening” complications developed during the third period of TD: pneumonia, endobronchitis, dysbiosis, and general lung injury syndrome (GLIS). On average, by Day 5, the MFS-SS index in these patients did not exceed 46 points, and the major life-supporting systems were in a state of compensation. There were no lethal outcomes in this subgroup of patients. A characteristic feature of the third period of trauma disease was the maintenance of the subcompensation state of the major life-supporting systems achieved during the second period.
In 44 patients from Group 2 with TD Type II, the disease progression differed somewhat from the Type I course described above. The second period of TD in Group 2 patients also became distinctly manifested on Day 2 after the injury, which was accompanied by the maintenance of the minimum value of the MFS-SS over a 10-day period — 47.5 ± 0.3 points. In the patients of this subgroup during this TD period, the systems of gas exchange, hemodynamics, and blood most frequently remained decompensated in various combinations; decompensation of liver function and the gastrointestinal tract also persisted, or marked endotoxicosis was present. The subsequent third period of TD in the patients of this subgroup was characterized not only by a persistent and prolonged increase in the severity of their condition but also by the development of life-threatening complications, such as severe sepsis (18.5%), septic shock (3.0%), acute respiratory distress syndrome (ARDS), generalized fibrinolysis (5.5%), fat embolism syndrome (1.8%), and pulmonary embolism (3.7%). The injury severity in the patients of this subgroup ranged 3.6–14.2 points on the MFS-I scale (averaging 10.3 ± 0.3 points), while the severity of the condition upon admission ranged 24.0–31.0 points on the MFS-SE scale (averaging 27.6 ± 0.4 points) (Table 1).
In 48 patients (Type III, Fig. 1), the TD course was the most severe. According to modern concepts, the injuries sustained by all these patients fell under the definition of “polytrauma”, i.e., they were the most severe and complex types of traumas with impairment of vital functions. The injury severity in this subgroup ranged 15.0–45.5 points on the MFS-I scale (averaging 18.5 ± 1.6 points). The minimum severity of the condition upon admission was 32.0 points on the MFS-SE scale, and the maximum was 75.0 points (averaging 43.4 ± 2.9 points) (Table 1).
The main feature of the first period of TD in this subgroup was high lethality. During this period, a lethal outcome occurred in 14.6% of the patients. The second period of TD in the subgroup of patients with polytrauma was indistinct (blurred); the MFS-SS index was 72.6 ± 4.3 points, with pronounced coagulopathy determining the severity of the general condition. The major life-supporting systems remained decompensated, with the exception of compensated metabolic acidosis. The third period in this subgroup was characterized by the development of life-threatening complications such as severe sepsis (20.8%) and acute respiratory distress syndrome (20.8%) [14].
Our MST methodology (Fig. 3) was proposed after studying the clinical and laboratory parameters of the patients involved in the study. The MST technique is based on the principles of the temporal progression of TD and the dependence of the TD type on the severity of impaired body functions. MST begins in the admission and triage department and is completed upon the discharge of the patient. Surgeons and ICU specialists face the decision regarding the necessity of performing tracheostomy and gastrostomy for effective management of patients with jaw fractures.

Figure prepared by the authors
Fig. 3. Algorithm of multistage surgical treatment: MFS-I — Military Field Surgery (Injury); MFS-I (MI) — Military Field Surgery (Mechanical Injury); MFS-SS — Military Field Surgery (Specialized State); TD — trauma disease; ICU — intensive care unit; MST — multistage surgical treatment
Note: * — calculation of the linear discriminant function (LDF) using formulas: LDF1 = 7.01Х1 + 1.34Х2 + 0.31Х3 – 10.42 и LDF2= 9.09 Х1 + 1.07Х2 + 0.17Х3 – 10.24, where Х1 — abs. lymphocyte count on Day 3, Х2 — Leukocyte Index of Intoxication (LII) on Day 3, Х3 — Injury severity according to the MFS-I (MI) scale; if LDF1 > LDF2 — positive prognosis for the development of purulent complications; if LDF1 < LDF2 — negative prognosis for the development of purulent complications.
For discussion, we propose a definition of an “abbreviated” MST protocol, which is implemented without tracheostomy or gastrostomy. In the admission and triage department, with an injury severity of 1.0–2.0 points, an abbreviated MST protocol is performed without tracheostomy, after which the patient is transferred to a specialized general care department. Following the performed surgeries (under emergency and urgent protocols), the severity of the general condition was assessed using the MFS-SS scale.
By the end of the first period of TD, patients in the first group showed an improvement in their general condition to 46 ± 0.48 points [15].
Under an injury severity of 2.0–12.0 points and decompensation of the general condition, Stage 1 MST is performed in full. In other variants, an abbreviated MST protocol without tracheostomy or gastrostomy is performed. With an injury severity > 12.0 points (averaging 18.8 ± 1 point), MST is performed in full (Fig. 3).
The conducted clinical and biometric studies allowed us to develop an MST protocol, which takes into account the injury severity and the level of compensation for impaired functions. The algorithm of the developed MST is presented in Figure 3.
In cases of the injury severity of 1.0–2.0 points and impaired body functions (MFS-SE scale score of 18.8 ± 0.9 points), under emergency indications, MST is performed using an abbreviated protocol without tracheostomy. Subsequently, patients are transferred to a specialized department where conservative management of the impaired functions is conducted during the 2nd and 3rd periods of TD. After full stabilization of the condition (MFS-SS score below 50 points), a scheduled operation to correct the anatomical changes is performed. Emergency surgeries are performed on the chest, abdomen, major vessels, pelvis, and extremities.
In cases of the injury severity of 2.0–12.0 points with decompensation of the general condition (MFS-SE scale score greater than 26.2 ± 0.8 points), an emergency operation is performed in a shock room, after which patients are transferred to an ICU.
In cases where the injury severity exceeds 12.0 points and impaired body functions (MFS-SE scale score of 42.2 ± 3.3 points) are present, Stage 1 of MST is performed in full. This includes:
These measures are carried out simultaneously in a shock room with support of specialists of other profiles. Subsequently, the patients are transferred to an ICU. Urgent surgeries are performed on the head and brain, chest, abdomen, pelvic organs, and major vessels. Delayed surgeries are also performed on the pelvic bones, spine, spinal cord, and long tubular bones.
This stage corresponds to the 2nd and 3rd periods of TD, lasting from Day 2 to Day 10. The patients are on prolonged mechanical ventilation and receive comprehensive infusion-transfusion and antibacterial therapy (from Day 5, therapy is adjusted based on microbiological monitoring results).
Starting from Day 3, a prognosis concerning the development of severe and extremely severe disease courses is made (according to the MFS-SS scale: 50–69 points — severe form of TD; 70–98 points — extremely severe form of TD). In cases of severe TD forms with a favorable outcome and a negative prognosis for the development of infectious complications, MST is performed using an abbreviated protocol. Starting from Days 4–10, based on bacterial culture results, targeted antibiotic therapy is administered along with minimally invasive surgeries (sanitation of potential sources of infectious complications). In certain cases, staged fixation of fragments is performed using minimally invasive external osteosynthesis.
In cases of an extremely severe form of TD with an unfavorable outcome, or with a favorable outcome but a positive prognosis for the development of infectious complications (calculated using the linear discriminant function (LDF) with two formulas, see note to Fig. 3), MST is performed in full. At this stage, exhaustive diagnostics of damaged structures using computed tomography (CT) is also carried out. Creation of conditions for functional rest for the damaged structures is a component of comprehensive treatment, including the use of enteral tubes via the piriform aperture or placement of a gastrostomy. The second period concludes upon the resolution of the patient’s complications and the normalization of the general condition to a level of compensation: below 50 points on the MFS-SS scale.
Bacteriological monitoring, antibacterial therapy, immunotherapy, immunocorrection, and surgical management of complications are applied.
This reconstructive and restorative stage corresponds to the 4th period of TD. Stage 3 can be initiated only after the complete stabilization of the patient’s general condition. Surgical interventions are performed in full in the specialized departments of a Level I trauma center (neurosurgery, maxillofacial surgery, traumatology, and other departments).
When conducting a comparative analysis, our data showed good agreement with those from the Military Field Surgery Department of the Kirov Military Medical Academy [1].
The conducted study allowed us to achieve the research objectives. An MST methodology for combined midface injuries, which takes into account the severity of trauma and impaired body functions, has been developed. The MST strategy for patients with combined midface trauma represents a set of surgical interventions that are implemented starting from the first day of admission and are completed with reconstructive and restorative operations.
Depending on the severity of injury and the nature of the TD course, the range of surgical interventions performed within the framework of MST is differentiated. In severe TD, the likelihood of immediate outcomes and the probability of visceral infectious complications are assessed. In cases where the immediate outcome is predicted to be favorable and the prognosis for the development of visceral infectious complications is negative, then MST is carried out according to a simplified, abbreviated protocol. In cases where the prognosis for immediate outcomes is unfavorable, or when the immediate outcome is favorable but visceral infectious complications are probable, MST is performed in full.
When studying the nature of TD course in patients with craniofacial trauma, its following types were established:
The implementation of the conventional protocol in 20 patients with extremely severe combined craniofacial injuries led to the development of infectious complications in 77.8% of cases, with lethality being observed in 44.4% of cases. The developed MST allowed a 47.7% reduction in the frequency of infectious complications and a 43.7% reduction in lethality to be achieved. Thus, among 22 patients with comparable injuries, infectious complications were noted in 41.6% (9 patients; p < 0.05), and lethality was 25% (5 patients; p < 0.001)).
The advantage of the developed MST strategy consists in an optimal scope of diagnostic and therapeutic measures, dynamically adapted to the progression of the pathological process, alongside the development and integration of modern technologies.
Authors’ contributions. All authors confirm that their authorship complies with the ICMJE criteria. The primary contributions are distributed as follows: Yurii A. Shcherbuk — responsibility for the management and coordination of research planning and execution; Olga D. Madai — data visualization, material processing, analysis of literary data, manuscript writing; Dmitrii Yu. Madai — article concept, design and conception of the clinical case, responsibility for the integrity of all parts of the article, text editing, final approval of the manuscript, final manuscript formatting, and responsibility for the management and coordination of research planning and execution; Alexandr Yu. Shcherbuk — draft editing.
1. Maday DYu. Choice of Surgical Treatment Strategy for Patients with Combined Injuries Depending on Injury Severity: Lecture. Saint Petersburg: Saint Petersburg State University Publishing House; 2010.
2. Sokolov VA. “Damage Control” — A Modern Concept for the Management of Patients with Critical Polytrauma. Lecture. Priorov Journal of Traumatology and Orthopedics. 2005.
3. Ivanov A.G. Content and Organization of Surgical Care for Maxillofacial Wounds in the Context of the Special Military Operation. Study Guide. Saint Petersburg: Saint Petersburg State University Publishing House.
1. Gumanenko YeK, Zavrazhnov AA, Suprun AYu, Khromov AA. Severe combined trauma and polytrauma: definition, classification, clinical characteristics, treatment outcomes. Polytrauma. 2021;4:6–17 (In Russ.). https://doi.org/10.24412/1819-1495-2021-4-6-17
2. Kharitonov DYu, Dmitriev VV, Stepanov IV, Podoprigora AV, Moiseeva VS, Garshina MA. Dependence of the severity of brain damage on the localization of facial fractures in patients with combined craniofacial injuries. Journal of New Medical Technologies. 2019;26(1):22–5 (In Russ.).
3. Fokas NN, Levenetc AA, Gorbach NA, Pavlushkin AA, Metelev IA, Kravtsova GN. Research methodology traumatic injuries maxillofacial (for example Krasnoyarsk Region). International Journal of Applied and Fundamental Research. 2015;10–5:826–9 (In Russ.). EDN: ULVDCR
4. Maslyakov VV, Barachevsky YuE, Pavlova ON, Proshin AG, Polikarpov DN, Pimenov AV, et al. Analysis of the results of treatment of combined and isolated injuries of the facial skull resulting from traffic accidents in regional trauma centers. Polytrauma. 2021;4:28–38 (In Russ.). https://doi.org/10.24412/1819-1495-2021-4-28-37
5. Belen’kiy IG, Manukovskii VA, Tulupov AN, Demko AE, Kandyba DV, Sergeev GD, et al. Strategies of Osteosynthesis: Problems and Perspectives. Traumatology and Orthopedics of Russia. 2022;28(2):79–90 (In Russ.). https://doi.org/10.17816/2311-2905-1693
6. Grebnev GA, Sviridenko AD, Krasikov AV. Comparative characteristics of classifications of injuries of the middle zone of the face. Russian Journal of Dentistry. 2021;25(4):307–13 (In Russ). https://doi.org/10.17816/1728-2802-2021-25-4-307-313
7. Pfeifer R, Kalbas Y, Pape H-C. The concept of “Damage control” in polytrauma: what are standards in 2021? Polytrauma. 2021;2:10–8 (In Russ.). https://doi.org/10.24412/1819-1495-2021-2-10-18
8. Pfeifer R, Kalbas Y, Coimbra R, Leenen L, Komadina R, Hildebrand F, et al. Indications and interventions of damage control orthopedic surgeries: an expert opinion survey. European Journal of Trauma Emergency Surgery. 2020;47:2081–92. https://doi.org/10.1007/s00068-020-01386-1
9. Abu-Zidan FM, Jawas A, Idris K, Cevik AA. Surgical and Critical Care Management of Earthquake Musculoskeletal Injuries and Crush Syndrome: A Collective Review. Turkish Journal of Emergency Medicine. 2024;24(2):67–79. https://doi.org/10.4103/tjem.tjem_11_24
10. Arnaouti MKC, Cahill G, Baird MD, Mangurat L, Harris R, Edme LPP, et al. Medical Disaster Response: A Critical Analysis of the 2010 Haiti Earthquake. Frontiers in Public Health. 2022;1(10):9955–95. https://doi.org/10.3389/fpubh.2022.995595
11. Tribble DR, Murray CK, Lloyd BA, Ganesan A, Mende K, Blyth DM, et al. After the Battlefield: Infectious Complications among Wounded Warriors in the Trauma Infectious Disease Outcomes Study. Military Medicine. 2019;184:18–25. https://doi.org/10.1093/milmed/usz027
12. Stewart L, Li P, Blyth DM, Campbell WR, Petfield JL, Krauss M, et al. Antibiotic practice patterns for extremity wound infections among blast-injured subjects. Military Medicine. 2020;185:628–36. https://doi.org/10.1093/milmed/usz211
13. McDonald J, Liang SY, Li P, Stewart L, Tribble DR. DoD-VA trauma infection research collaboration. Military Medicine. 2022;187:17–24. https://doi.org/1010.1093/milmed/usab508
14. Trajano AD, Pereira BM, Fraga GP. Epidemiology of in-hospital trauma deaths in a Brazilian university hospital. BMC Emergency Medicine. 2014;14:22. https://doi.org/10.1186/1471-227X-14-22
15. Roberts DJ, Bobrovitz N, Zygun DA, Kirkpatrick AW, Ball CG, Faris PD, et al. Evidence for use of damage control surgery and damage control interventions in civilian trauma patients: a systematic review. World Journal of Emergency Surgery. 2021;16(1):10. https://doi.org/10.1186/s13017-021-00352-5
Yurii A. Shcherbuk, Dr. Sci. (Med.), Academician of RAS, Professor
St. Petersburg
Olga D. Madai, Cand. Sci. (Med.), Associate Professor
St. Petersburg
Dmitrii Yu. Madai, Dr. Sci. (Med.), Professor
St. Petersburg
Alexandr Yu. Shcherbuk, Dr. Sci. (Med.), Professor
Moscow
Shcherbuk Yu.A., Madai O.D., Madai D.Yu., Shcherbuk A.Yu. Multistage surgical management of patients with combined craniofacial injuries. Extreme Medicine. 2026;28(1):123-133. https://doi.org/10.47183/mes.2025-375
10 bld. 1 Pogodinskaya Str., Moscow, Russia 119121
tel.: +7 (495) 540-61-71, ext.: 4190, 4191, 4192
E-mail: Extrememedicine@cspfmba.ru
Processing of personal data











