



Contents
Scroll to:
https://doi.org/10.47183/mes.2024-26-3-51-56
Scroll to:
Introduction. Considering the risks of cardiovascular events during all phases of spaceflight (SF), it is relevant to evaluate the levels of cardiac markers sST2 and NT-proBNP in ground-based simulations of exposure to adverse SF factors.
Objective. To identify the levels of sST2 and NT-proBNP as risk criteria for the development of cardiovascular changes following end-to-end simulation of SF stages on the CF-18 centrifuge.
Materials and methods. The levels of cardiac markers sST2 and NT-proBNP were assessed during exposure to chest-to-back overloads of up to 4.5 units and simulated vestibular sensory conflict on a CF-18 centrifuge for 60 min in six healthy male subjects. The sST2 levels were assessed by solid-phase enzymelinked immunosorbent assay (ELISA). NT-proBNP concentration was measured by immunofluorescence method on a Finecare TM FIA FS-113 analyzer (from Guangzhou Wondfo Biotech).
Results. During the end-to-end simulation of SF stages, the response of the subjects’ cardiovascular system was adequate to the loads imposed. The levels of the cardiac markers sST2 and NT-proBNP in venous blood of the subjects did not significantly increase after spinning on the centrifuge.
Conclusions. In the present study, no significant changes indicative of biochemical signs of pathologic overstretching or myocardial damage were observed during rotation on the CF-18. Assessment of individual sST2 levels prior to exposure and in dynamics can be used to probabilistically predict individual sensitivity and adaptation reserves of the heart to unfavorable CP factors.
Goncharova A.G., Kireev K.S., Pastushkova L.Ch., Kashirina D.N., Goncharov I.N., Larina I.M. Assessment of soluble sST2 and NTproBNP cardiac markers during end-to-end stimulation of space flight stages on a long radius centrifuge. Extreme Medicine. 2024;26(3):51-56. https://doi.org/10.47183/mes.2024-26-3-51-56
Ensuring the medical safety of space flights and medical control of health status is a priority task in space medicine. A comprehensive health status assessment for predicting the risks of acute and remote cardiovascular events involves the application of highly informative clinical and laboratory techniques. Soluble growth stimulators are known to be expressed by gene 2 (sST2) in cardiomyocytes in response to their overstretching or damage [1]. Unlike other cardiac markers, sST2 levels change rapidly in response to the subject’s cardiovascular status but are independent of age, sex, body mass index, and renal function [2][3]. SST2 has been shown to be the most significant marker for predicting the development and outcome of heart failure [4].
sST2 levels were evaluated during parabolic flights in the context of aerospace physiology. Significantly decreased serum sST2 levels compared to values at baseline and 1 h after parabolic flight were observed to remain unchanged 1 h after parabolic flight [5]. In earlier studies, we analyzed the effects of long-duration space flight (SF) and landing on sST2 protein levels. In the study of venous blood samples of nine astronauts before and after SF to the International Space Station, all subjects showed a significant increase in sST2 level on the first day after the flight. On the 7th day of the recovery period, the sST2 content in plasma decreased to approach the background value. The obtained results indicated transient myocardial overstretching during landing and increased risk of cardiofibrosis over the long term following SF [6].
Another standard cardiac marker of cardiac volume overload and risk of heart failure and cardiac rhythm disturbances is the N-terminal propeptide of natriuretic hormone (B-type) NT-proBNP [7]. However, NT-proBNP is dependent on age, sex, body mass index, daily hormone balance, renal status, and other factors [8]. Considering gravitational features of NT-proBNP regulation, we note that individual astronauts showed a decrease in natriuretic peptide signaling while in space [9]. As shown in Frings-Meuthen P, et al. [10], NT-proBNP concentrations respond to changes in sodium intake under SF conditions, but have lower levels relative to preflight values. This appears to occur due to decreased blood volume in the thoracic cavity provided that impedance measurements are not distorted by changes in chest air content.
We were interested in whether short-term overload and vestibular sensory changes simulated on a CF-18 centrifuge would influence pathologic myocardial extensibility and increase the risk of cardiac fibrosis. Thus, the purpose of the present study was to determine the levels of sST2 and NT-proBNP in relation to the risk of cardiovascular changes in vestibular sensory changes following end-to-end simulation of SF stages on a CF-18 centrifuge.
Experimental investigations (EI) were carried out at the Gagarin Research and Test Cosmonaut Training Center in 2023 according to the method described earlier [11]. The study involved six practically healthy male subjects aged 45 to 53 years (mean age 50.3 ± 3.3 years, height 175.7 ± 4.7 cm, body mass 86.8 ± 6.7 kg). All subjects were medically cleared for EI and had a valid medical and flight commission report.
A medical examination of the subjects with registration of cardiovascular system functional parameters (blood pressure BP, heart rate HR) and body temperature was carried out by a physician before and after the EI. Prior to the study, the subjects had not been exposed to other influences that could affect their functional state and postural reactions (physical activity, acceleration, negative or excessive pressure on the lower half of the body, hypoxia). Studies were conducted no earlier than 1.5 h after a meal. All subjects received detailed instructions for all stages of the study.
The EIs were performed on a CF-18 centrifuge for physiological studies with a cabin installed in a 3-stage controlled gimbal. The radius of the centrifuge console from the rotation axis of the main engine to the center of intersection of the gimbal frames axes is 18 m. The studies were conducted using the standard seat of the centrifuge СF-18. Under these conditions, the overload acts in the chest-back direction. During the ascent and descent phases, the inclination angle of the seat back to the direction of the overload vector was +78°. Following simulation of the 3rd stage engine separation, the subject’s chair was moved to a position at 105° from the direction of the overload vector (anti-orthostasis –15°) and the orbital space flight stage was simulated. Rotations were performed without stopping the centrifuge.
During the rotation on the CF-18, a tacho-oscillographic method was used to monitor the electrocardiogram (ECG) in three standard leads, as well as HR and BP in the brachial artery.
Figure 1 shows a typical profile of overloads influencing the cosmonaut during the Soyuz ascent into Earth orbit (“ascent schedule”), while Figure 2 shows a typical profile of overloads during the Soyuz descent to Earth (“descent schedule”). The overload is stated in multiple units of gravity acceleration (g). The maximum overload during rotation according to the “descent schedule” is 4.0 units; the total rotation time is about 9 min. The overload during the “descent schedule” rotation includes two sections with a maximum overload of 4.5 units (peak 1) and 3.2 units (peak 2) involving a total rotation time of about 6 min. Simulation of the orbital flight stage for 40 min was performed using a special program [11], which provides simultaneous changes in hemodynamics and impact on the vestibular apparatus of the tester. The total duration of rotation was 60 min.
While ECG was recorded in three standard leads in the centrifuge cabin before, during and after rotation, brachial artery BP was performed using tacho-oscillographic method. During centrifuge rotation, ECG was recorded continuously. At the same time, BP was recorded at the 10th, 20th, 30th and 40th minutes of rotation.
To determine the concentration of sST2 and NT-proBNP, venous blood was sampled from the ulnar vein of the subjects immediately before and after rotation. Blood samples of 3 mL were collected before and at the end of rotation into Vacuette® tubes containing K3 EDTA preservative. Following storage in blood tubes at +4°C for no more than 2 h, plasma was obtained by centrifugation at 2000 g for 15 min on an MPW-350R centrifuge (Poland); plasma aliquots were sampled using the Eppendorf (Germany) interchangeable volume pipettes. Plasma aliquots were frozen at –80°C.
The sST2 level in blood plasma was assessed by solid-phase enzyme-linked immunosorbent assay (ELISA) using commercial kits of “Critical Diagnostics Presage® ST2 Assay” (USA) and ST2-reader “Critical Diagnostics Presage® ST2 Assay”. The results of sST2 level measurement were expressed in ng/mL. NT-proBNP concentration was measured according to the immunofluorescence method on a FinecareTM FIA FS-113 analyzer (from Guangzhou Wondfo Biotech). Statistical processing of the experimental data was carried out using the Statistica 13 software package based on Friedman’s analysis of variance criterion and the Wilcoxon test for nonparametric data (p-value < 0.05).
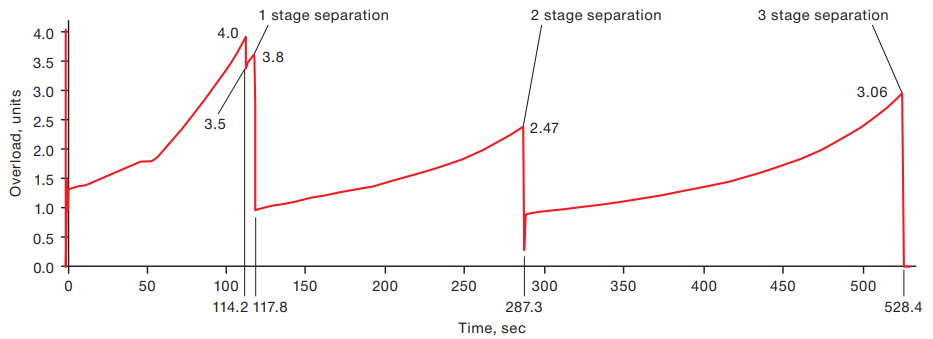
Figure prepared by the authors using their own data
Fig. 1. Typical overload profile during the Soyuz ascent
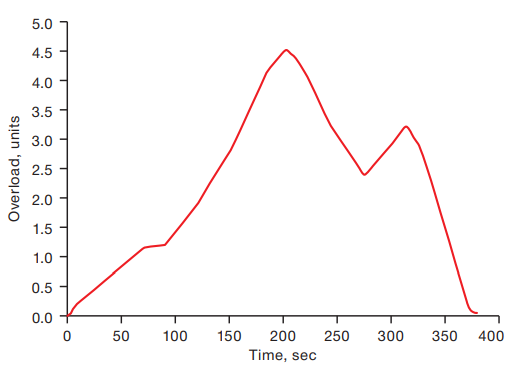
Figure prepared by the authors using their own data
Fig. 2. Typical overload profile during the Soyuz descent
During the medical examination of the subjects before the EI, the mean values of systolic BP were 138.9 ± 11.2 mmHg, diastolic BP was 85.0 ± 9.9 mmHg, mean HR was 74.8 ± 16.9 beats/min, body temperature in all subjects was within the physiologic norm. All subjects were admitted to the EI.
From the first min of orbital flight stage modeling and transfer to the anti-orthostatic position during periodic questioning while rotating, all six subjects subjectively noted blood rush to the head, four reported the sensation of facial swelling and heaviness in the temporal region of the head, three mentioned nasal congestion, two described cold feet, and one reported heavy eyelids. During rotation under video observation, mild hyperemia of the facial skin and swelling of neck veins were objectively observed in all test subjects. The severity of all phenomena rose with increasing duration of rotation to reach a maximum by 20 min and remained unchanged thereafter.
The dynamics of changes in cardiovascular system parameters are presented in Figure 3 and Figure 4.
The response of the cardiovascular system was adequate to the loads imposed. The maximum registered values of HR and BP corresponded to the maximum overloads at each simulated stage of space flight.
When analyzing the ECG during the simulation of the orbital flight section, in most cases the subjects registered an increase in the end part of the ventricular QRS complex and in the amplitude of the T tooth; at the same time, the RST interval was slightly shortened. In isolated cases, a slowing of intraventricular conduction was detected, as expressed in “broadening” of the ventricular complex. These changes, which were functional in nature, disappeared after stopping the TF. Sinus tachycardia was noted during rotations according to the “withdrawal schedule” and “descent schedule”; there were no rhythm or conduction disturbances.
A medical examination following the EI did not reveal any deviations in the state of health. No subjects had any complaints; their general well-being remained positive. Hemodynamic parameters did not significantly differ from background. Average values of systolic BP were 143.2 ± 14.1 mmHg, diastolic BP was 82.6 ± 19.3 mmHg, mean values of HR were 71.7 ± 15.9 beats/min, while body temperature remained within normal limits.
As can be seen from Figure 5, sST2 levels did not exceed the reference values in any test subject. Variability of sST2 levels was noted in all subjects both prior to the modeling and following its completion. When analyzing the group-average sST2 levels, its increase following rotation on the TF was noted (Fig. 6). However, the level of group-average values after exposure to overloads also fell within the reference values (variant of physiological norm up to 35 ng/mL). The obtained data indicate the absence of risks of heart failure and cardiofibrosis under the described study conditions.
As shown in Figure 7, the variability of NT-proBNP before and after modeling remains low. Individual variability is higher than the group average (Figures 7 and 8). NT-proBNP levels remained within the normal range at all investigated points in all test subjects.
When comparing individual and mean group graphs of response of cardiac markers sST2 and NT-proBNP to this type of exposure, attention was paid to unidirectional increase of sST2 and NT-proBNP levels after exposure in 4 out of 6 subjects. However, the NT-proBNP level increased less than sST2.
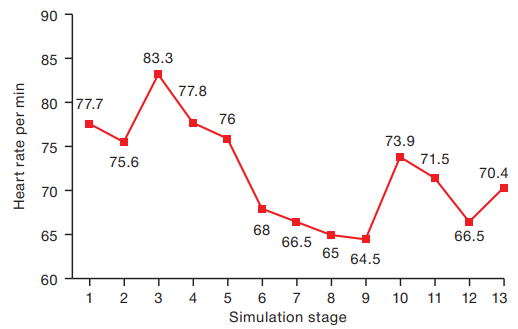
Figure prepared by the authors using their own data
Fig. 3. Heart rate dynamics during simulation of the space flight stages: 1 — baseline before simulation; 2 — beginning simulation; 3 — 1st stage separation; 4 — 2nd stage separation; 5 — 3d stage separation; 6 — 10th min of orbital flight; 7 — 20th min of orbital flight; 8 — 30th min of orbital flight; 9 — 40th min of orbital flight; 10 — 1st overload peak during Soyuz landing; 11 — 2nd overload peak during the Soyuz landing; 12 — end of simulation; 13 — 5 min after end of simulation
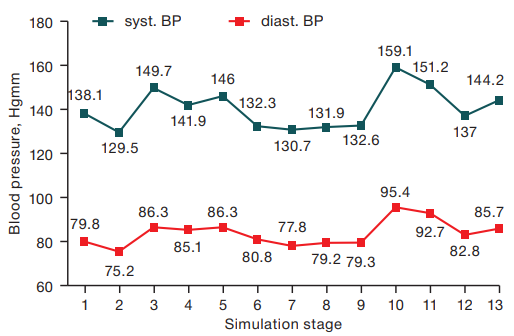
Figure prepared by the authors using their own data
Fig. 4. Blood pressure dynamics during simulation of the space flight stages: 1 — baseline before simulation; 2 — beginning simulation; 3 — 1st stage separation; 4 — 2nd stage separation; 5 — 3d stage separation; 6 — 10th min of orbital flight; 7 — 20th min of orbital flight; 8 — 30th min of orbital flight; 9 — 40th min of orbital flight; 10 — 1st overloads peak during Soyuz landing; 11 — 2nd overloads peak during the Soyuz landing; 12 — end of simulation; 13 — 5 min after end of simulation
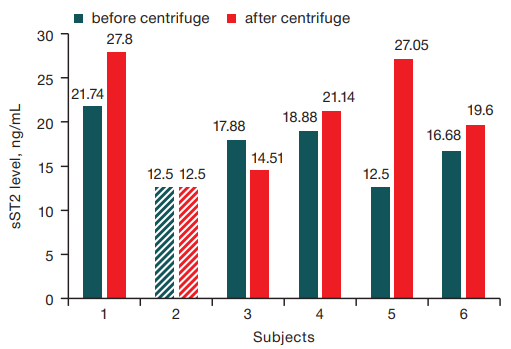
Figure prepared by the authors using their own data
Fig. 5. Individual sST2 levels before and after simulation of the space flight stages. Note: sST2 levels below the sensitivity of the method (<12,5 ng/mL) are marked with a dash
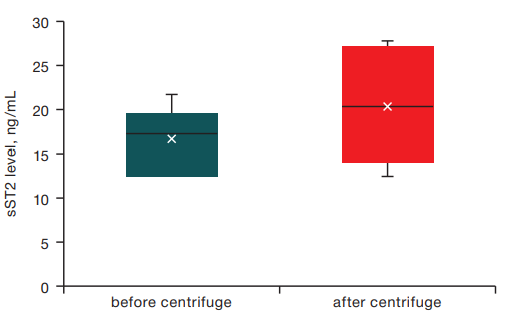
Figure prepared by the authors using their own data
Fig. 6. Mean group sST2 levels before and after simulation of the space flight stages
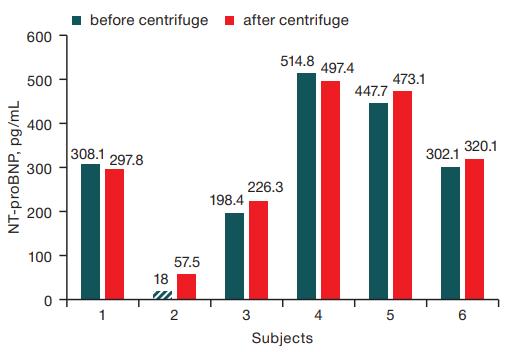
Figure prepared by the authors using their own data
Fig. 7. Individual NT-proBNP levels before and after simulation of the space flight stages. Note: NT-proBNP levels below the sensitivity of the method (<18 pg/mL) are marked with a dash
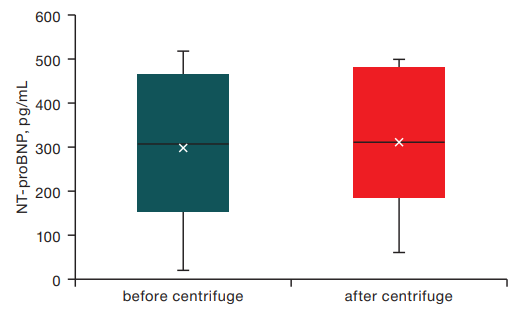
Figure prepared by the authors using their own data
Fig. 8. Mean group NT-proBNP levels before and after simulation of the space flight stages
From the analysis of the obtained data, the dynamics of heart rate and blood pressure level was seen to correspond to the applied loads. Maximal registered values of HR and BP observed at maximal impacting overloads at each simulated SF stage did not exceed physiological values of variability of responses of cardiovascular system of a healthy person to the impact of simulated extreme factors of SF. The in-depth study of cardiomyocyte response to the effect of moderate longitudinal overloads on the myocardium of practically healthy subjects showed a unidirectional increase in the levels of cardiac markers sST2 and NT-proBNP, which confirms the high diagnostic sensitivity of these proteins with respect to even short-term effects causing volumetric overstretching of myocardium. Analysis of individual data showed a more pronounced and variable response to overload exposure of the selective cardiac marker sST2 as compared with NT-proBNP. Multimarker models comprised of several biomarkers, including NT-proBNP and sST2, have greater prognostic significance for risk stratification of cardiovascular events [12–14]. Thus, changes in sST2 and NT-proBNP can objectively characterize the response of cardiomyocytes to the effect of overload both at active sites of SF according to ascent and descent schedules and at modeling of redistribution of body fluid media in microgravity conditions. Based on estimation of individual background levels of sST2 and NT-proBNP, it is also possible to personalize probabilistic prognosis of the effect of the complex of SF factors at the stage of orbital insertion and descent in order to estimate the risk of cardiofibrosis development in remote periods after SF.
In contrast to earlier studies of sST2 level after completion of prolonged SF [6], the present study did not reveal a clinically significant increase in the level of this cardiac marker following completion of space flight stage simulation on a CF-18. The obtained data indicate that isolated exposure of the myocardium of practically healthy subjects to moderate longitudinal overload without prior exposure to prolonged microgravity does not cause pathologic overstretching of cardiomyocytes. The increase in sST2 level following prolonged SF can be explained by the effect of overloads during the descent vehicle return to the Earth on myocardia that are already adapted to the prolonged influence of extreme SF factors [15].
1. Weinberg E, Shimpo M, de Keulenaer G. W, MacGillivray C, Tominaga S, Solomon S. D, et al. Expression and regulation of ST2, an interleukin-1 receptor family member, in cardiomyocytes and myocardial infarction. Circulation. 2002;106(23):2961–6. https://doi.org/10.1161/01.cir.0000038705.69871.d9
2. Uchasova EG, Gruzdeva OV, Dileva YuA, Karetnikova VN. Interleukin 33 and fibrosis: pathogenesis updated. Medical Immunology. 2018;20(4):477–84 (In Russ.). https://doi.org/10.15789/1563-0625-2018-4-477-484
3. Dudek M, Kałużna-Oleksy M, Migaj J, Straburzyńska-Migaj E. Clinical value of soluble ST2 in cardiology. Adv Clin Exp Med. 2020;29(10):1205–10. https://doi.org/10.17219/acem/126049
4. Rehman S, Mueller T, Januzzi JL. Characteristics of the novel interleukin family biomarker ST2 in patients with acute heart failure. J Am Coll Cardiol. 2008;52(18):1458–65. https://doi.org/10.1016/j.jacc.2008.07.042
5. Jirak P, Wernly B, Lichtenauer M, Paar V, Franz M, Knost T, et al. Dynamic Changes of Heart Failure Biomarkers in Response to Parabolic Flight. Int J Mol Sci. 2020;21(10):3467. https://doi.org/10.3390/ijms21103467
6. Goncharova AG, Pastushkova LKh, Kireev KS, Kashirina DN, Goncharov IN, Koloteva MI, Larina IM. Influence of the Factors of Long-Duration Space Flights and Landing on the Levels of Cardiac Failure Biomarker and sST2 Fibrosis Development Risk. Manned Spaceflight. 2023;46(1):96–103 (In Russ.). https://doi.org/10.18127/j15604136-202301-06
7. Cao Z, Jia Y, Zhu B. BNP and NT-proBNP as Diagnostic Biomarkers for Cardiac Dysfunction in Both Clinical and Forensic Medicine. Int J Mol Sci. 2019;20(8):1820. https://doi.org/10.3390/ijms20081820
8. Maries L, Manitiu I. Diagnostic and prognostic values of B-type natriuretic peptides (BNP) and N-terminal fragment brain natriuretic peptides (NT-pro-BNP). Cardiovasc J Afr. 2013;7:286–9. https://doi.org/10.5830/CVJA-2013-055
9. Rössler A, Noskov V, László Z, Polyakow VV, Hinghofer-Szalkay HG. Permanent depression of plasma cGMP during long-term space flight. Physiol Res. 2001;50:83–90.
10. Frings-Meuthen P, Luchitskaya E, Jordan J, Tank J, Lichtinghagen R, Smith SM, et al. Natriuretic Peptide Resetting in Astronauts. Circulation. 2020;141(19):1593–5. https://doi.org/10.1161/CIRCULATIONAHA.119.044203
11. Kireev KS, Zaveryukha AS, Vlasova NV, Minyaylo YaYu, Gavrik IN, Bulgakov AV, Dubinin VI. The study of cosmonauts’ functional status during the end-to-end simulation of space-flight phases on the centrifuge TSF-18. Manned Spaceflight. 2024;51(2):63–78 (In Russ.). EDN: AFLTPG
12. Gaggin HK, Truong QA, Gandhi PU, Motiwala SR, Belcher AM, Weiner RB, et al. Systematic evaluation of endothelin 1 measurement relative to traditional and modern biomarkers for clinical assessment and prognosis in patients with chronic systolic heart failure: serial measurement and multimarker testing. Am J Clin Pathol. 2017;147(5):461–72. https://doi.org/10.1093/ajcp/aqx014
13. Ky B, French B, Levy WC, Sweitzer NK, Fang JC, Wu AH, et al. Multiple biomarkers for risk prediction in chronic heart failure. Circ Heart Fail. 2012;5(2):183–90. https://doi.org/10.1161/CIRCHEARTFAILURE.111.965020
14. Lupon J, de Antonio M, Vila J, Penafiel J, Galan A, Zamora E, et al. Development of a novel heart failure risk tool: the Barcelona bio-heart failure risk calculator (BCN bio-HF calculator). PLoS One. 2014;9(1):e85466. https://doi.org/10.1371/journal.pone.0085466
15. Sy MR, Keefe JA, Sutton JP, Wehrens XHT. Cardiac function, structural, and electrical remodeling by microgravity exposure. Am J Physiol Heart Circ Physiol. 2023;324(1):H1–H13. https://doi.org/10.1152/ajpheart.00611.2022
Moscow
Zvyozdny Gorodok
Moscow
Moscow
Moscow
Moscow
Goncharova A.G., Kireev K.S., Pastushkova L.Ch., Kashirina D.N., Goncharov I.N., Larina I.M. Assessment of soluble sST2 and NTproBNP cardiac markers during end-to-end stimulation of space flight stages on a long radius centrifuge. Extreme Medicine. 2024;26(3):51-56. https://doi.org/10.47183/mes.2024-26-3-51-56
10 bld. 1 Pogodinskaya Str., Moscow, Russia 119121
tel.: +7 (495) 540-61-71, ext.: 4190, 4191, 4192
E-mail: Extrememedicine@cspfmba.ru
Processing of personal data











